ICL (Intraocular Collamer Lens)
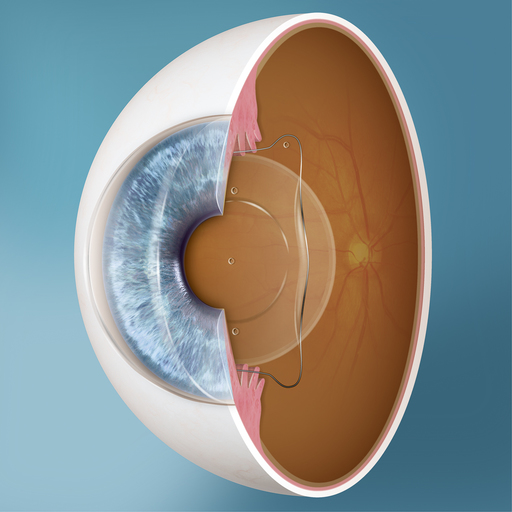
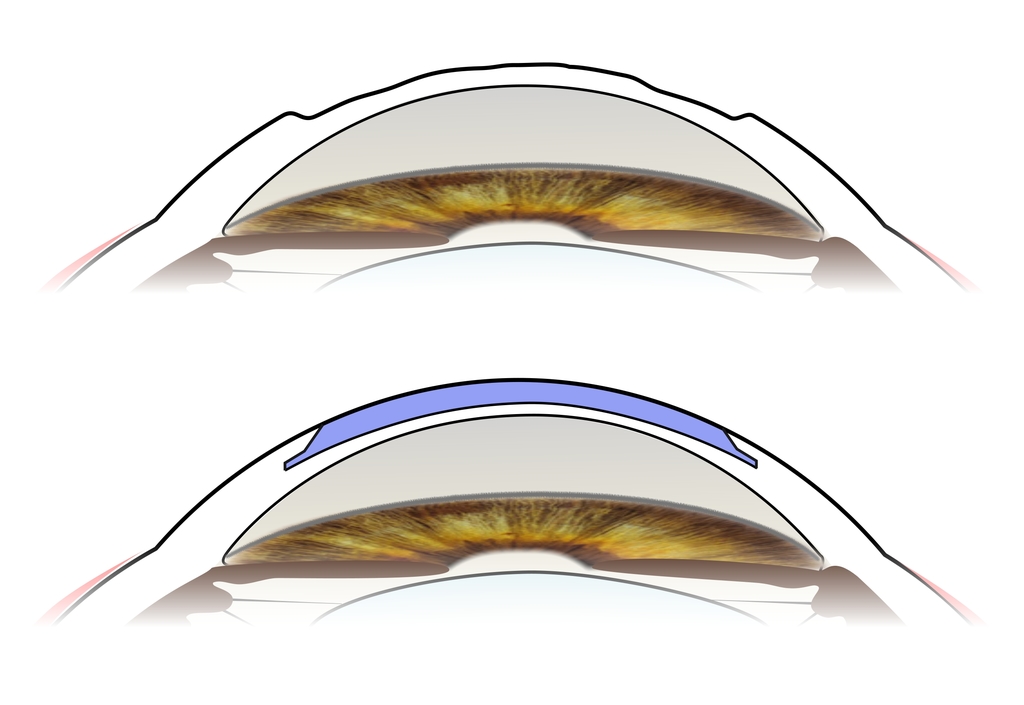
The implantable collamer lens (ICL) is a lens designed to rest in front of the natural human lens of the eye floating on an aqueous layer. This lens is called the VISIAN EVO+ ICL and is made of an advanced collamer lens material that is highly biocompatible with the eye. It is a co-polymerisation product of hydrophobic and hydrophilic acrylic material polymerised with telo-collagen. It has excellent UV blocking incorporated, is soft and elastic allowing gentle implantation by the surgeon. The lens is not normally felt by the recipient when implanted within the eye.
The lens has a low refractive index, so it does not back reflect or glint and is normally invisible to an observer.
The ICL has been in use since 1993 and over the past 31 years there has been improvement in manufacturing technology and design, so the current model has a much bigger optical zone than previously, which helps night vision.
The ICL is available up to -18.0 D with up to 6 Dioptres of astigmatism. For eyes with more extreme refractive error and optical distortions limiting vision it is possible to perform a wavefront-guided excimer laser custom treatment to treat residual refractive error. This is termed “bioptics”.
The ICL lens design features the “KS-Aquaport”, which is a small central hole in the lens optic that facilitates aqueous flow and eliminates the need to make a small hole in the iris (iridectomy). This has minimised or eliminated risk of aqueous flow blockage and appears to prevent anterior cataract development which could previously occur with phakic lens implants. The central drainage hole can induce early halos and glare, but in 95% of cases, they reduce significantly or disappear in the first 3 to 6 months after implantation. There are some people who still see haloes after ICL implantation when the pupil is very large at night, and this is due to some light coming into the eye around the edge of the ICL lens.
The ICL is preferred over corneal excimer laser eye surgery (PRK or LASIK) or SMILE where there is higher refractive error. It is also favoured where there is significant dry eye or where there is a thin or irregular cornea and laser eye correction may be contraindicated.
The ICL can reduce or eliminate total dependence on glasses or contact lenses. ICL and wavefront-guided surface treatment or LASIK all have the potential to provide very high quality of vision. Generally, the bigger the intended treatment the more the ICL is favoured. An alternative is to continue to use glasses or contact lenses.
ICL vision correction is becoming increasingly popular and there have been over 2 million ICL lenses implanted worldwide.
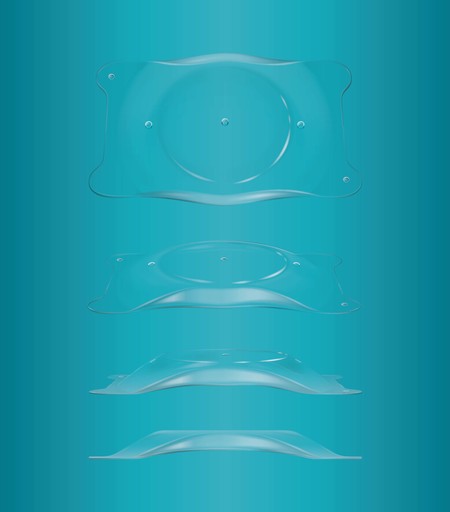
The ICL lens is low refractive index and is transparent
ICL Information 2025
Corneal transplantation
As a specialist corneal surgeon, Mr Stevens performs corneal transplantation, including femtosecond laser lamellar and penetrating keratoplasty corneal transplantation.